
Holmium Laser Enucleation of the Prostate (HoLEP)
HoLEP is an advanced, minimally invasive procedure that uses a high-powered holmium laser to precisely remove obstructive tissue from an enlarged prostate.
Advanced Holmium Laser Prostate Surgery
The ability to urinate normally can be significantly affected by an enlarged prostate as its increased size puts pressure on the urethra and bladder. Leading to symptoms such as a decrease in the flow rate of the urine, or frequently needing to get up and urinate during the night.
Holmium Laser Enucleation of the Prostate (HoLEP) is an advanced and minimally invasive procedure which helps to relieve these symptoms by removing obstructive prostate tissue using a high-energy Holmium Laser.
The Urology Partnership are experts and nationally recognised trainers for HoLEP surgery offering patients relief from urinary symptoms due to benign prostatic hyperplasia (BPH).
To discuss your suitability, or possible alternatives, please contact our Reading Clinic on 0118 920 7040.
Advantages of HoLEP
In this short video, urology consultant Mr Sunil Kumar explains the benefits HoLEP offers patients.
- Recommended for very large prostates: HoLEP is particularly useful for larger prostates (over 80-100cc). It removes more prostate tissue than a TURP would but with less chance of bleeding and a shorter recovery time. There is an added advantage of also doing vapourisation, resection or a combination of vapo-resection with the Holmium Laser.
- Advanced procedure: HoLEP is the most advanced laser technique currently available and has been recommended by the National Institute of Clinical Excellence (NICE) in its guidelines.
- Highly effective: In contrast to Green Light Laser Vapourisation of the prostate, HoLEP has been rigorously evaluated in randomised trials. It is a size independent procedure suitable for any prostate in experienced hands, and highly effective at treating urinary retention.
- Very low blood loss: The high power Holmium Laser separates the central part of the prostate from the surrounding fibrous covering (capsule), and this procedure is nearly bloodless as when the laser beam cuts the gland it also seals the blood vessels.
Holmium Laser Enucleation of the Prostate (HoLEP) Procedure
What happens during the HoLEP procedure
HoLEP is usually carried out under a general anaesthetic and takes around 60-180 minutes, depending on the size of your prostate.
The procedure is performed with a special endoscope passed through the urethra. During surgery the high-energy Holmium Laser is used to remove the core of the prostate from inside the gland to create an open channel, whilst avoiding the muscles and nerves that are important to maintain urinary continence and erectile function.
The removed prostate tissue is pushed into the bladder, and a special instrument (morcellator) is then used through a telescope device to remove the tissue. A sample of the removed tissue is then sent for biopsy to check for any signs of prostate cancer. Once complete, a temporary catheter is inserted to help the bladder drain normally.
You’ll stay in over-night and the catheter will be removed the next day, after which you’ll be able to return home.
Recovering after HoLEP
Recovery time: Most patients feel tired and below par for a week or two. We recommend 3-4 weeks rest before resuming any job, especially if it is physically strenuous. You should also avoid any heavy lifting during this time.
Expect some bleeding: There is always some bleeding from the prostate area after the operation. The urine is usually clear of blood within 10 to 14 days.
Discomfort passing urine: At first, it may be painful to pass your urine and it may come more frequently than normal. Any initial discomfort can be relieved by painkillers such as Paracetamol and the frequency usually improves within a few days.
Passing prostate tissue: You may notice that you pass very small flecks of tissue in the urine at times within the first month as the prostate area heals. This does not usually interfere with the urinary stream or cause discomfort.
A gradual reduction in symptoms: The symptoms of an overactive bladder (frequency, urgency, getting up at night to pass urine) may take three months to resolve, whereas the flow is improved immediately.
Pelvic floor exercises: There may be some temporary loss of urinary control until your pelvic floor muscles strengthen and recover. Starting pelvic floor exercises as soon as possible after the operation can improve your control.
Sexual activity: Removal of your prostate should not adversely affect your erections provided you are getting normal erections before the surgery. However, the surgery often result in dry ejaculation. Sexual activity can be resumed as soon as you are comfortable; usually after 3-4 weeks.
Driving after surgery: You can resume driving after surgery once you feel fit and able.
Potential HoLEP complications
As with any other medical procedure there is a potential for side effects such as bleeding, blood clots, pain or difficulty passing urine.
In most cases the HoLEP procedure is performed successfully. However, possible complications may include:
- Dry ejaculation
- Increase in urinary frequency and urgency
- Infection of the bladder, testes or kidney
- Loss of urinary control (incontinence)
- Erectile dysfunction (poor erections)
- Infertility (unable to produce semen during orgasm)
- Scarring of the urethra (urethral stricture)
- Prostate regrowth
Private HoLEP surgery at The Urology Partnership
At The Urology Partnership, we understand the importance of timely and expert urological care. Our team of specialists is dedicated to providing you with fast access to an excellent, patient-centred service, in a caring and comfortable private clinic environment.
Contact us today to arrange a consultation with one of highly experienced urology consultants to discuss your suitability for HoLEP surgery.
Call: 0118 920 7040
Email: info@theforburyclinic.co.uk
Location: The Forbury Clinic, 11 Kendrick Road, Reading, Berkshire.
Holmium Laser Enucleation of the Prostate (HoLEP) FAQs
There are a number of alternative treatment options for a benign enlarged prostate (BPH) which we offer at The Urology Partnership.
These include medication, use of a catheter to bypass the obstruction, observation, conventional transurethral resection (TURP) surgery or an open operation.
There are some newer alternatives such as Robotic Aquablation, Rezum, Urolift and Prostate Artery Embolisation (PAE).
The suitability of these procedure options can be discussed with your consultant during your appointment.
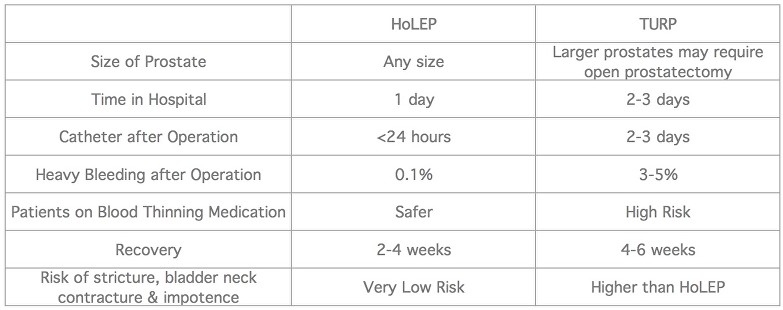
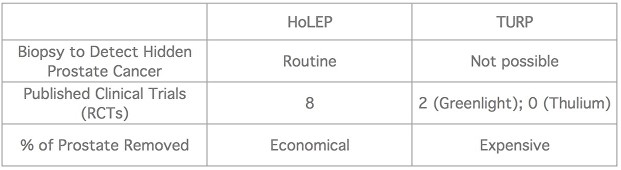
Compared to TURP, HoLEP offers a number of advantages:
Fixed priced quotes available on request. Please contact us on 0118 920 7040.
For further information on the HoLEP procedure you may be interested in finding out more via the following external resources
National Institute of Clinical Excellence, NICE
BAUS (British Association of Urological Surgeons) Patient Information Sheet
Laser Prostatectomy, Wikipedia
Prostate Laser Surgery, The Mayo Clinic, USA
Royal Berkshire Hospital HoLEP. Patient Information Sheet
Next Steps
Get fast access to leading specialists for the swift diagnosis and treatment of urological conditions in a private clinic environment.
If you would like more information or wish to arrange a consultation with one of our specialist consultant urological surgeons then please either Call 0118 920 7040 or complete the form below.
Insured patients
Contact your GP and ask for a referral to the Urology Partnership.
All consultations, investigations and treatments are covered by major insurance companies (depending on policy).
Funding your own treatment
Self-funding initial consultation fee is £250. Follow up fees are £175.
Consultation charges are exclusive of any tests and other investigations that the consultant may wish to carry out.